Rising Painkiller Addiction Shows Damage From Drugmakers’ Role in Shaping Medical Opinion
Below is the latest in the Washington Post series–Can Medical Research be Trusted? its focus is the continued rise in painkiller addiction and the decisive role played by corrupt pharmaceutical marketing practices.
Of note, more than a decade ago, in 2002, the US Drug Enforcement Administration (DEA) reviewed medical examiners’ toxicology reports from 32 states. The DEA reported that OxyContin was involved in 464 overdose deaths, few included alcohol consumption.
But, over much of the past decade, the official word on OxyContin was that it rarely posed problems of addiction for patients. The label on the drug, which was approved by the FDA, said the risks of addiction were “reported to be small.”The New England Journal of Medicine, the nation’s premier medical publication, informed readers that studies indicated that such painkillers pose “a minimal risk of addiction.” Another important journal study, which the manufacturer of OxyContin reprinted 10,000 times, indicated that in a trial of arthritis patients, only a handful showed withdrawal symptoms.
· Those reassuring claims, which became part of a scientific consensus, have been quietly dropped or called into question in recent years, as many in the medical profession rediscovered the destructive power of opiates. But the damage arising from those misconceptions may have been vast.
· The nation is confronting an ongoing epidemic of addiction to prescription painkillers — more widespread than cocaine or heroin — that has left nearly 2 million in its grip, according to federal statistics.
“Around here, we call it ‘pharmageddon,’ ” said Lisa Roberts, the public health nurse for the town, whose primary job is to reduce the fatalities associated with drug use. “This has been absolutely devastating to Appalachia. From what we’ve seen, the risks of addiction were tremendous.”
· “It turns out that the doctors didn’t know what they were talking about,” said Barbara Howard, whose daughter Leslie, a home-care nurse, died of an overdose in 2009 in this small Appalachian town devastated by the epidemic. She had developed a habit after knee surgery. She left behind a 9-year-old son.
· “Leslie trusted the doctors. We thought the doctors knew what was best. But they didn’t. We — and lots of the other victims — had no warning.”
“You could say these marketing tactics are merely concerning. But I think of them as satanic. What the data are telling us is that these drugs are ruining people’s lives,” said Phillip Prior, MD
To refine its policy on opioids, the FDA convened a key meeting in 2002 and invited 10 outside experts for advice. Five of them reported having served as speakers or investigators for Purdue. Three others reported working as speakers for or as advisers and consultants to other pharmaceutical companies.
One of those FDA advisers, Dr. Russell Portenoy, who was then the chair of the Department of Pain Medicine and Palliative Care at the Beth Israel Medical Center in New York, has since expressed regret for his evangelism on behalf of opioids.
He was “trying to create a narrative so that the primary care audience would . . . feel more comfortable about opioids,” Portenoy said in a 2010 interview, “Because the primary goal was to destigmatize [opioids], we often left evidence behind.
“To the extent that some of the adverse outcomes now are as bad as they have become in terms of endemic occurrences of addiction and unintentional overdose deaths, it’s quite scary to think about how the growth in that prescribing driven by people like me led in part to that occurring.”
In 2003, Purdue Pharmaceuticals, the manufacturer of OxiContin–whose sales reached $1.3 billion–had the gall to sponsor advertisements warning about prescription drug abuse!
Vera Sharav
~~~~~~~~~~~~~~~~~~~~~~~~~~
THE WASHINGTON POST
Special Report: Can medical research be trusted?
A Washington Post investigation finds pharmaceutical companies influence the research that determines drug prescriptions for millions of Americans.
- Bingeing on prescription painkillers
- Antidepressants to treat grief?
- As drug industry’s influence over research grows, so does the potential for bias
- Medicare overspending on anemia drug
- Anemia drug made billions, but at what cost?
- Graphic: The rise and fall of a billion-dollar drug
By Peter Whoriskey,
Rising painkiller addiction shows damage from drugmakers’ role in shaping medical opinion
December 30, 2012 

Michelle Davis with picture of sister, Gail Phok who diedfrom prescription drug (Photos by Joel Prince/ For The Washington Post )
Portsmouth, Ohio — Over much of the past decade, the official word on OxyContin was that it rarely posed problems of addiction for patients.The label on the drug, which was approved by the FDA, said the risks of addiction were “reported to be small.”
The New England Journal of Medicine, the nation’s premier medical publication, informed readers that studies indicated that such painkillers pose “a minimal risk of addiction.”
Another important journal study, which the manufacturer of OxyContin reprinted 10,000 times, indicated that in a trial of arthritis patients, only a handful showed withdrawal symptoms.
Those reassuring claims, which became part of a scientific consensus, have been quietly dropped or called into question in recent years, as many in the medical profession rediscovered the destructive power of opiates. But the damage arising from those misconceptions may have been vast.
The nation is confronting an ongoing epidemic of addiction to prescription painkillers — more widespread than cocaine or heroin — that has left nearly 2 million in its grip, according to federal statistics.
“It turns out that the doctors didn’t know what they were talking about,” said Barbara Howard, whose daughter Leslie, a home-care nurse, died of an overdose in 2009 in this small Appalachian town devastated by the epidemic. She had developed a habit after knee surgery. She left behind a 9-year-old son.“Leslie trusted the doctors. We thought the doctors knew what was best. But they didn’t. We — and lots of the other victims — had no warning.”
 Conflicts of interest
Conflicts of interest
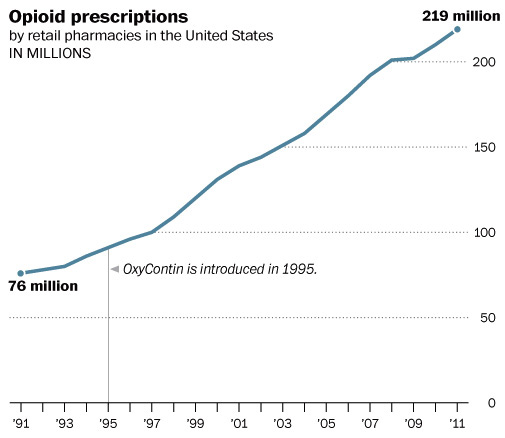
A closer look at the opioid painkiller binge — retail prescriptions have roughly tripled in the past 20 years — shows that the rising sales and addictions were catalyzed by a massive effort by pharmaceutical companies to shape medical opinion and practice.
Opioids are a class of powerful drugs, often used for pain, that includes morphine, heroin and brand names such as OxyContin, Vicodin and Percocet.
For years, doctors had been cautious about prescribing opioids to anyone except patients with cancer or in acute pain.
But drug manufacturers and some pain specialists helped create a body of scientific research assuaging the long-standing worries about opioids and pushed to expand the use of the drugs in people with chronic pain — bad backs, arthritis, sore knees.
Their studies reported minimal risks of addiction and dependence. These, in turn, were accepted by the FDA and the nation’s medical journals. State medical boards made their rules for prescribing opioids more liberal. Academic and industry articles dismissed the old fears as “opiophobia.”
These reports reached doctors through marketing efforts and told them that there were few risks in using opioids to treat chronic pain.
But according to a Washington Post examination of key scientific papers, a court document and FDA records, many of those claims were developed in studies supported by Purdue Pharma, the maker of OxyContin, or other drug manufacturers. In addition, the conclusions they reached were sometimes unsupported by the data, and when the FDA was struggling to come up with an opioid policy, it turned to a panel populated by doctors who had financial relationships with Purdue and other drugmakers.
· A review of 16 key clinical trials on the subject shows that five were funded by Purdue and an OxyContin distributor, two were co-authored by Purdue employees, and two were sponsored by other drug companies making different opioids. None of the 16studies showed clear warnings about the addiction dangers or the physical dependence generated by the drugs. The low rate of addiction reported in these studies is at odds with more recent findings indicating that diagnoses of addiction are common in opioid patients.
· Internal company documents indicate that one of the key published studies sponsored by Purdue — the one reprinted 10,000 times — omitted suspected cases of withdrawal symptoms. The published paper offered assurance that only two of more than 100 OxyContin patients had withdrawal symptoms; the internal documents showed that at least 11 exhibited possible signs of withdrawal, and some experts say it is likely that at the doses given, most of the patients would have experienced withdrawal.
· To refine its policy on opioids, the FDA convened a key meeting in 2002 and invited 10 outside experts for advice. Five of them reported having served as speakers or investigators for Purdue. Three others reported working as speakers for or as advisers and consultants to other pharmaceutical companies.
One of those FDA advisers, Russell Portenoy, who was then the chair of the Department of Pain Medicine and Palliative Care at the Beth Israel Medical Center in New York, has since expressed regret for his evangelism on behalf of opioids. 
He was “trying to create a narrative so that the primary care audience would . . . feel more comfortable about opioids,” Portenoy said in a 2010 interview with Andrew Kolodny, the chief of a group seeking to rein in drug use, Physicians for Responsible Opioid Prescribing. “Because the primary goal was to destigmatize [opioids], we often left evidence behind. . . .
“To the extent that some of the adverse outcomes now are as bad as they have become in terms of endemic occurrences of addiction and unintentional overdose deaths, it’s quite scary to think about how the growth in that prescribing driven by people like me led in part to that occurring.”
Through a spokesman, Portenoy declined to comment for this report, but he has said that he continues to believe that many patients with chronic pain can benefit from opioids, though the estimates of how many patients may become addicted are larger than previously thought.
At the time of the 2002 FDA meeting, Portenoy reported being a speaker for Purdue Pharma. He also reported involvements on contracts and grants with Parke-Davis, Boehringer Ingelheim, Elan, Ortho Biotech, Endo, Ametek, Medtronic, Purdue Pharma, Pfizer, Janssen, Abbott, Curatech, Ortho-McNeil and Searle.
James Heins, a spokesman for Purdue, said that “it is implausible that our marketing caused an upsurge in overall prescriptions of opioids or in the incidence of abuse” because the company commands only a small portion of the painkiller market. Moreover, he said, the notion that the risk of addiction was small was “not based on studies funded by Purdue but rather on the larger body of medical literature and clinical experience.”Even today, he said, it is difficult to say exactly how many people who are prescribed opioids become addicted.
‘Absolutely devastating’
In few places are the effects of the opioid epidemic clearer than in Portsmouth, a town near Ohio’s borders with West Virginia and Kentucky. About 10 percent of babies are born addicted to opioids. At one point, nine “pill mills” operated out of this region of 80,000 people. About 20 people a year die of drug overdoses. Last year, for every resident, more than 100 doses of opioids were prescribed and dispensed.
Ask someone here whether the risks of opioid addiction are minimal, and some snort or roll their eyes. “Around here, we call it ‘pharmageddon,’ ” said Lisa Roberts, the public health nurse for the town, whose primary job is to reduce the fatalities associated with drug use. “This has been absolutely devastating to Appalachia. From what we’ve seen, the risks of addiction were tremendous.”
For decades, many doctors had been wary of prescribing opioids except for use by cancer patients and the terminally ill. In 1992, for example, a survey of state medical board members, most of them physicians, found that only 12 percent described prescribing opioids for an extended period for chronic pain as a “lawful and generally acceptable medical practice.”
Advocates for opioid prescription, backed in part by drugmakers, set about seeking to change those attitudes. More than 20 states changed their rules. And in December 1995, these marketing efforts surged as Purdue Pharma introduced OxyContin, a controlled-release form of the opioid oxycodone.
From 1996 to 2000, the company doubled its sales force from 300 to 671, according to a 2003 report by what was then the General Accounting Office. The amount of sales bonuses Purdue Pharma offered tied to OxyContin grew from $1 million a year to $40 million a year. It sponsored pain-related Web sites, advertised in medical journals and paid influential doctors such as Portenoy to talk to other physicians.
As the number of overdoses and reports of addicts rose in the early 2000s, key questions arose. How were the addicts becoming addicted? Was it by going to the doctor with a legitimate pain and getting a legitimate prescription? Or was it just people seeking a high and buying the prescription drugs off the street?
If it was only the latter, limiting prescriptions might have little direct effect on the problem and could penalize pain sufferers. But it was both. Although many addicts started on opioids just to get high, experts say, a good portion arrived at their habits after coming into contact with opioids after a doctor’s visit for a legitimate pain. That’s how Leslie Cooper came to the drug, and it is reportedly the way some celebrities became addicted: Rush Limbaugh, Matthew Perry, Cindy McCain.
Other trials have reported that significant numbers of pain patients are addicted. In one review out of Yale School of Medicine, investigators found that diagnoses of addiction are “common” in patients given opioids for back pain, with as many as 24 percent engaging in “aberrant” or peculiar ways of taking the pills.
Early on, officials at the Drug Enforcement Administration perceived the danger to patients.
“The company’s aggressive methods, calculated fueling of demand and the grasp for major market share very much exacerbated OxyContin’s widespread abuse and diversion,” a November 2003 memo from the agency said. “The claim in Purdue’s ‘educational’ video for physicians that opioid analgesics cause addiction in less than one percent of patients is not only unsubstantiated but also dangerous because it misleads prescribers.”
But amid the marketing blitz, concerns about addiction in patients appear to have faded from the medical profession.
The FDA, which must approve drug labels, allowed Purdue to say on its label: “The development of addiction to opioid analgesics in properly managed patients with pain has been reported to be rare.”
The agency warned that drug abusers and addicts might try to obtain the drugs, but it indicated that the risks seemed minor for patients: “We do not know how often patients with continuing (chronic) pain become addicted to narcotics, but the risk has been reported to be small.” The agency, however, would later change its mind.
By 2008, the claims that the risks of addiction in patients were small were removed from the OxyContin label, after “extensive negotiations” with Purdue, an FDA spokeswoman said. “The labeling information, including language regarding addiction, has evolved over time as data has become available,”Morgan Liscinsky said. The FDA did not say what evidence led the agency to allow the previous claims or what new findings led it to ask for the removal of those claims.
Early on, however, the agency relied on industry experts for advice. In the 2002 FDA meeting, for example, eight of the 10 invited experts had connectionswith pharmaceutical companies. Of those, five had served as speakers, consultants or investigators for Purdue, including Portenoy and Kathy Foley, a neuro-oncologist at Memorial Sloan Kettering Cancer Center. Together, Portenoy and Foley had published a key study on opioids in 1986 that found that only two of 38 patients seemed to abuse the drugs and that both had histories of substance abuse.
“Their past work with industry should not preclude them from sharing their expertise with government agencies or their peers in the medical community,” Heins, the Purdue spokesman, said.
The FDA and doctors also could turn to a spate of other trials that seemed to suggest there was little reason to worry that chronic pain patients could get addicted to opioids. Take, for example, a 2003 report in the New England Journal of Medicine, which reviewed the conclusions from several studies. “The general finding is that patients with chronic pain . . . can achieve satisfactory analgesia . . . with a minimal risk of addiction,” it said, while questioning the use of high doses.
What may be most striking about the paper, though, is that its lead author has become one of the top critics of opioid prescribing habits. But Jane Ballantyne, a pain specialist at the University of Washington, said that at the time there were very few clinical trials that showed any sign of an addiction risk.
“There were very few studies then that suggested that any more than 8 percent of people on prescription opioids exhibited addiction-type behaviors,” Ballantyne said. Now, she said, the understanding is that the number may be as high as 50 percent.
How did all these studies — co-authored by doctors with university affiliations and published in academic journals — lead to conclusions that now are in dispute? One reason, according to critics, is that most of the studies were conducted by drug companies.
“A pharmaceutical company that has a vested interest in promoting their product should not be seen as a reliable source of safety information,” said Orman Hall, director of the Ohio Department of Alcohol and Drug Addiction Services. “Some of those estimates are ludicrous.”
Consider the 16 clinical trial reports that Ballantyne highlighted and used in her article, which reflect the medical literature at the time. Her summary did not discuss sponsors of the studies. But of those 16, six were sponsored by Purdue Pharma or co-authored by its employees, one was sponsored by Mundipharma, which distributed OxyContin and other opioids, and two were sponsored by another drug company or co-authored by drug company employees.
In the trials, patients were given an opioid for pain, but in most, there were no systematic checks for withdrawal symptoms or addiction. Instead, in most of the trials, regardless of whether they were sponsored by drug companies, the investigators generally found that the benefits of pain relief outweighed the risks of side effects such as constipation and dry mouth.
If investigators were looking for signs of addiction, they weren’t looking hard. “In the absence of rigorous evaluation and surveillance, it’s hard to know whether the low levels of addictive behavior reported in those studies are accurate,” said David A. Fiellin, a professor of medicine at Yale with an expertise in addiction.
Fiellin noted that the design of a study can dramatically change the results and that entrusting the design to scientists with conflicts of interest could introduce bias. What patients are admitted to the trial? How are side effects measured? How large are the doses?
“All of those are scientific decisions that should be made by people without any regard for how the findings will affect the company’s bottom line,” Fiellin said, adding that the government could play a larger role in funding.
Data discrepancy
In one of the studies sponsored by Purdue that Ballantyne covered, and that played a large role in the marketing of OxyContin, there appear to have been significant discrepancies between the data that were gathered and those that were published.
A March 2000 issue of the Archives of Internal Medicine published a study that followed 106 arthritis patients treated with OxyContin for several months. Six times during the trial, researchers intentionally stopped the doses. Remarkably, according to doctors who study addiction and dependence, there were no reports of withdrawal during those respites. Two patients had withdrawal problems, but one was at the end of the study, and the other had simply run out of the medication.
“Withdrawal syndrome was not reported as an adverse event for any patient during the scheduled respites,” the authors reported.
The trial also showed that the drug was effective and was embraced by the Purdue marketing team, which ordered 10,000 reprints to distribute to its sales staff, with instructions to highlight the finding on withdrawal.
But according to company documents disclosed in a court case, the paper left out several cases of withdrawal.
Inside Purdue, supervisors and employees reviewed a more complex set of data, according to a document signed by company attorneys and prosecutors, which accompanied a 2007 settlement in which federal prosecutors charged Purdue with misbranding the drug.The document has not previously been linked to the Archives article.
“Multiple” patients, a company review said, “directly stated or implied that an adverse experience was due to possible withdrawal symptoms.”
Eleven study patients “reported adverse experience due to possible withdrawal symptoms during these periods,” according to the court document.
How did this discrepancy arise?
One of the authors of the Archives article, Roy Fleischmann, a clinical professor of medicine at the University of Texas Southwestern Medical Center at Dallas, said the authors were given the data by Purdue. “We reported on the data which was provided to us,” he wrote.
He said the discrepancy may have arisen because some of the side effects — such as insomnia, nausea and anxiety — were not characterized by Purdue “as withdrawal symptoms, although, in retrospect, they probably were,” he said in an e-mail.
Doctors who have treated OxyContin addicts, and some former addicts, moreover, say that considering the doses given to the patients in the trial and its duration, even the internal document undercounted patients reporting withdrawal symptoms. They say the majority of patients were likely to have suffered withdrawal symptoms when the drug was cut off.
At the doses given in the trial, most patients are “pretty consistently” going to have withdrawal symptoms, said Phillip Prior, a board-certified addictionologist in the Portsmouth area who has treated thousands of patients addicted to opioids. He said the lower estimates are “flawed conclusions from a very flawed study.”
“I’ve never seen anyone come off of them and not get withdrawal,” said Billie Taylor, 42, a former addict who works at a treatment center in Portsmouth. “I would have quit a lot earlier if it had not been for the withdrawal. You feel like you want to die. Even if you take them at prescribed levels, you get withdrawal.”
“You could say these marketing tactics are merely concerning,” Prior said. “But I think of them as satanic. What the data are telling us is that these drugs are ruining people’s lives.”
- Bingeing on prescription painkillers
- Antidepressants to treat grief?
- As drug industry’s influence over research grows, so does the potential for bias
- Medicare overspending on anemia drug
- Anemia drug made billions, but at what cost?
- Graphic: The rise and fall of a billion-dollar drug
