
How a False Hydroxychloroquine Narrative Was Created
- The problem with Hydroxychloroquine, a drug with a 70-year safety track record, is that there is no profit to be made from this cheap, off-patent drug!

It is remarkable that a series of events taking place over the past 3 months produced a unified message about hydroxychloroquine, and produced similar policies about the drug in the US, Canada, Australia, NZ and western Europe. The message is that generic, inexpensive hydroxychloroquine is dangerous and should not be used to treat a potentially fatal disease, Covid-19, for which there are no (other) reliable treatments.
- Hydroxychloroquine had been used safely for 65 years in millions of patients. And so the message was crafted that the drug is safe for its other uses, but dangerous when used for Covid-19. It doesn’t make sense, but it seems to have worked.
1. You stop doctors from using the drug in ways it is most likely to be effective (in outpatients at onset of illness). You prohibit use outside of situations you can control.
2. You prevent or limit use in outpatients by controlling the supply of the drug, using different methods in different countries and states. In NY state, by order of the governor, hydroxychloroquine could only be prescribed for hospitalized patients. France has issued a series of different regulations to limit prescribers from using it. France also changed the drugs’ status from over-the-counter to a drug requiring a prescription.
3. You play up the danger of the drug, emphasizing side effects that are very rare when the drug is used correctly. You make sure everyone has heard about the man who died after consuming hydroxychloroquine in the form of fish tank cleaner.
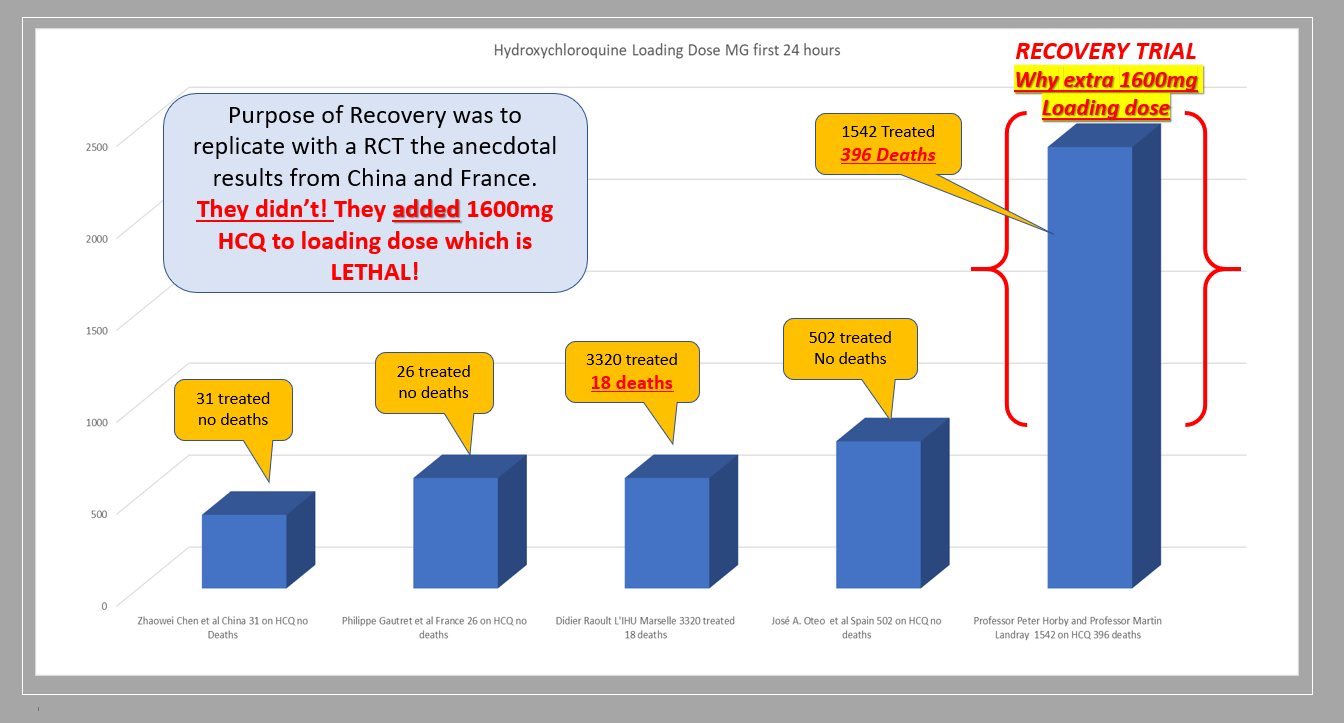
- Toxicity was noted after only 3 days of treatment, during which 3.6 grams of chloroquine were administered. But the Solidarity (3.2 grams of hydroxychloroquine in 3 days), Recovery (3.6 grams of hydroxychloroquine in 3 days) and REMAP-Covid trials (3.6 grams of hydroxychloroquine in 3 days) continued overdoing patients until June, despite Brazil’s evidence of deaths by overdose.
- Tellingly, JAMA editor Gordon Rubenfeld wrote about the Brazilian study, “if you are prescribing HCQ after these JAMA results, do yourself and your defense lawyer a favor. Document in your medical record that you informed the patient of the potential risks of HCQ including sudden death and its benefits (???).”

20. You have the head of the Coronavirus Task Force, Dr. Tony Fauci, insist the drug cannot be used in the absence of strong evidence…while he insisted exactly the opposite in the case of the MERS coronavirus outbreak several years ago, when he recommended an untested drug combination for use…which had been developed for that purpose by his agency.
And while he was bemoaning the lack of evidence, he was refusing to pay for trials to study hydroxychloroquine. And he was changing the goalposts on the Remdesivir trial, not once but twice, to make Remdesivir show just a tiny bit of benefit, but no mortality benefit. And don’t forget, Fauci was thrilled to sponsor a trial of a Covid vaccine in humans before there was any data from animal trials. So much for requiring high quality evidence before risking use of drugs and vaccines in humans!
21. You convince the public that the crisis will be long-lasting. You have the 2nd richest man in the world, and biggest funder of the WHO, Bill Gates, keep repeating to the media megaphone that we cannot go back to normal until there is a vaccine. (The Gates Foundation helped design the WHO clinical trials, and Gates is heavily invested in pharmaceuticals and vaccines.)

- You have CDC (with help from FDA) prevent the purchase of coronavirus test kits from Germany, China, WHO, etc, and fail to produce a valid test kit themselves. The result was that during January and February, US cases could not be reliably identified, and for several months thereafter insufficient and unreliable test kits made it impossible to track the epidemic and stop the spread.
- You have trusted medical spokesmen lie to the public about the pandemic’s severity, so precautions weren’t taken when they might have been more effective and less long-lasting. Congress was repeatedly briefed about the pandemic in January and February, which scared several Congress members enough that they sold off large amounts of stock, risking insider trading charges. Senator Burr is one of them, currently under investigation for major stock sales on February 13.
Yet Dr. Fauci told USA Today on February 17 that Americans should worry more about the flu than about coronavirus, the danger of which was “just miniscule.” Then on February 28, Drs. Fauci and Robert Redfield (CDC Director) wrote in the New England Journal:
“…the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
-
Professor Didier Raoult, MD, PhD You destroy the reputation of respected physicians who stand in your way. Professor Didier Raoult and his team in Marseille have used hydroxychloroquine on over 4,000 patients, reporting a mortality rate of about 0.8%. (The mortality rate of patients given hydroxychloroquine in the Recovery trial was 25.7%.) Raoult is very famous for discovering over 100 different microorganisms, and finding the long-sought cause of Whipple’s Disease. With this reputation, Raoult apparently thought he could treat patients as he saw fit, which he has done, under great duress. Raoult was featured in a New York Times Magazine article, with his photo on the cover, May 12, 2020. After describing his accomplishments, the Times very unfavorably discussed his personality, producing a detailed hit piece. He is now considered an unreliable crank in the US.
- You have social media platforms ban content that does not agree with the desired narrative. As YouTube CEO and ex-wife of Google founder Sergey Brin, Susan Wojcicki said,
“YouTube will ban any content containing medical advice that contradicts World Health Organisation (WHO) coronavirus recommendations. Anything that would go against World Health Organisation recommendations would be a violation of our policy.”
 When your clinical trials are criticized for overdosing patients, you have Oxford-affiliated, Wellcome Trust-supported scientists at Mahidol University publish papers (a literature review with modeling and a modeling study) purporting to show that the doses used were not toxic. You develop a new method to measure hydroxychloroquine in a handful of Recovery patients who were not poisoned. However, there are 2 problems you forgot with this approach:
When your clinical trials are criticized for overdosing patients, you have Oxford-affiliated, Wellcome Trust-supported scientists at Mahidol University publish papers (a literature review with modeling and a modeling study) purporting to show that the doses used were not toxic. You develop a new method to measure hydroxychloroquine in a handful of Recovery patients who were not poisoned. However, there are 2 problems you forgot with this approach:
- The Brazilian data, including 16 deaths, extensive clinical information and documented ventricular arrhythmias, are much more valuable than theoretical models of what might be happening in the body.
- Either the drug is too toxic to use for a life-threatening disease, or even extremely high doses are safe.
- You can’t have it both ways.
Oxford is the institution running the Recovery trial, and invented a Covid vaccine that already has 400 million doses on order. The Wellcome Trust funded the Recovery trial.
- You change your trial’s primary outcome measures after the trials have started, in order to prevent detection of drug-induced deaths (Recovery) or to make your drug appear to have efficacy (NIAID Remdesivir trial).
- You stop manufacturers from supplying the drug. Shortly after the fraudulent Lancet paper came out,
Sanofi announced it would no longer supply the drug for use with Covid, and would halt its two hydroxychloroquine clinical trials. One of the cancelled Sanofi trials was expected to test 210 outpatients early in the course of disease. The trial remains suspended at the time of writing, while the Lancet paper was retracted 13 days after publication. - You surely don’t want a trial of hydroxychloroquine treatment early in the disease, since it might show an excellent effect.


